Attendance tracking in medical education serves as a crucial foundation for developing professional responsibility and clinical competence. During the preclinical years, consistent attendance helps students build the comprehensive knowledge base required for patient care. This is achieved through structured learning experiences and real-time interaction with expert faculty. Medical education is collaborative. In case-based learning sessions and problem-based learning, each student’s presence enhances the collective learning environment. Students have valuable peer discussions. They challenge each other’s understanding. They develop the communication skills essential for their future roles as healthcare providers.
The early stages of medical training are particularly critical. They establish patterns of professional behavior and these patterns carry forward into clinical practice. Group learning activities, such as anatomy lab sessions and clinical skills workshops, require full participation to simulate the team-based nature of healthcare delivery. These sessions often cannot be adequately replicated through recorded lectures, independent study, or even as virtual sessions, as they rely on immediate feedback, hands-on practice, and the development of interpersonal skills. Regular attendance also allows faculty to identify struggling students early and provide necessary support, ensuring that future physicians develop the robust foundation of knowledge and skills required for safe and effective patient care.
Attendance tracking is surprisingly challenging in medical education. Many schools don’t use traditional learning management systems like Canvas or Blackboard that have built-in attendance tools. They prefer products that cater to health professions education like Elentra, One45, or MedHub. Medical education differs from other fields. There are 10s to 100s of different faculty members involved in teaching students over their medical careers. In contrast, language arts might only have one instructor for an entire semester. This is mainly due to the standard practice of having experts teach (e.g., a hiatal hernia specialist might teach a lecture on hernias). It can also be common to have 4-6 different faculty members team-teach a case-based lesson as each brings specific knowledge to share with the students. The point is that when there is one main instructor, keeping track of attendance is likely easier.
Some schools utilize technology to automate attendance tracking. At my school (University of Miami Miller School of Medicine), we use technology (iClicker) & rely on paper attendance forms for small group sessions. These sessions are in smaller classrooms and are led by individual facilitators. They pass out the paper forms and students sign their names. After the small group session, they provide the filled out attendance to the program manager who then updates rosters. As I am typing this, I realize how convoluted this sounds! It is convoluted and there are many reasons for it which maybe I’ll go into more detail in another post.
The Solution?
I am the co-chair of the Education Technology Work Group (ETWG). It is part of the American Association of Medical Colleges (AAMC) Group on Information Resources (GIR). This is a very vibrant group of dedicated #EdTech experts in medical schools from across the country. One of the benefits of being co-chair is having the opportunity to influence the topics we discuss. Recently, the topic for our monthly call was attendance tracking. Secretly, I hoped one school would share what they do. I imagined everyone on the call would nod in agreement with happy smiles. They would think that school has The Answer to the problem. Unfortunately, no one had a perfect solution. There is something comforting about experiencing the same issues, even if we don’t have the answers…yet.
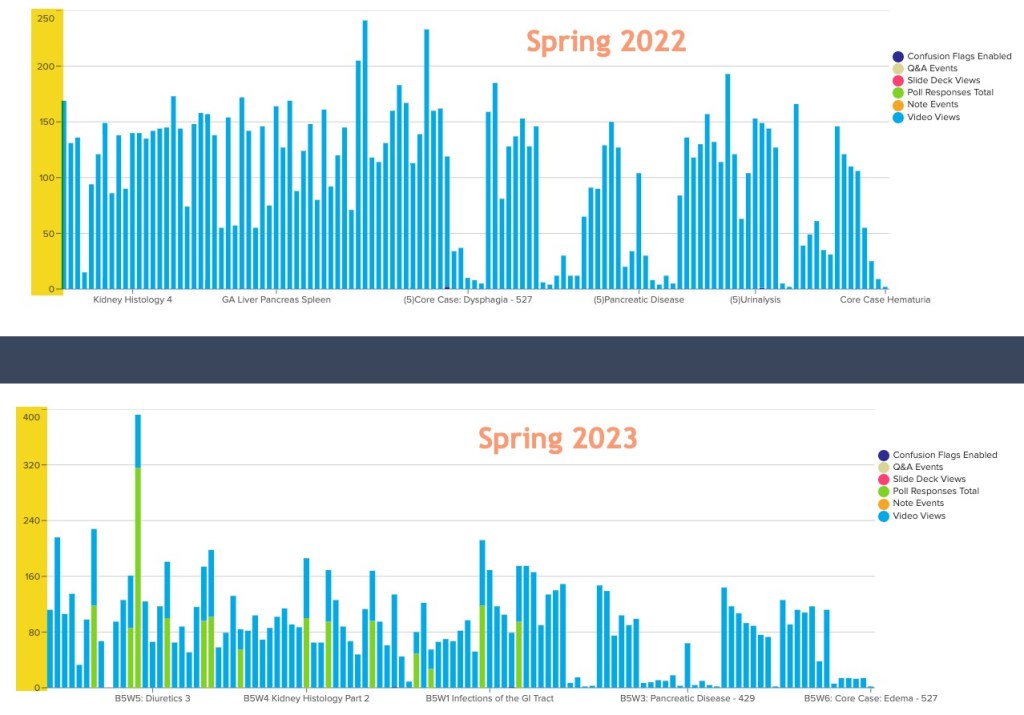
At MPOW (my place of work), we use a technological solution for the large group sessions. iClicker is our current solution and interfaces via LTI to our LMS, Blackboard. It’s not perfect. It has a dashboard for students to view their absences. They are limited to a certain number of them each semester so they want to be sure it’s accurate. There is not a way for students to contest absences in the dashboard. iClicker is mainly used for polling though it has attendance tracking functionality. We are looking at Qwickly as a possible replacement and fortunately, it also has an LTI with Blackboard. The same issue plagues Quickly though – there is a dashboard for students to review their attendance / absences, but there is not a way within the program for students to request a review or contest an absence.
So, we’ll do a pilot of it and see if it works any differently than iClicker and if not, there’s no reason to switch programs.
There’s a lot more to be said about the inclusion of technology in general in medical education, requiring attendance at all, and the blending of the two.
Further Reading
Amjad Ali Khan, U. M. (2024). Correlation of Academic Performance with Student Attendance in Pre-Clinical and Clinical Years of Undergraduate Medical Education. J. Islamic Int. Med. Coll., 18(4), 279–285. https://doi.org/10.57234/jiimc.december23.1692
Campbell, A. M., Ikonne, U. S., Whelihan, K. E., & Lewis, J. H. (2019). Faculty perspectives on student attendance in undergraduate medical education. Advances in Medical Education and Practice, 10, 759–768. https://doi.org/10.2147/AMEP.S208960
Kay, D., & Pasarica, M. (2019). Using Technology to Increase Student (and Faculty Satisfaction with) Engagement in Medical Education. Advances in Physiology Education, 43(3), 408–413. https://doi.org/10.1152/advan.00033.2019
Mandar Chandrachood. (2023). Revitalizing Classroom Attendance: Reviving Interest in Medical Education by Tackling Challenges and Embracing Solutions. GAIMS Journal of Medical Sciences, 4(1), 1–2. https://doi.org/10.5281/zenodo.8212557